Blog Details
Home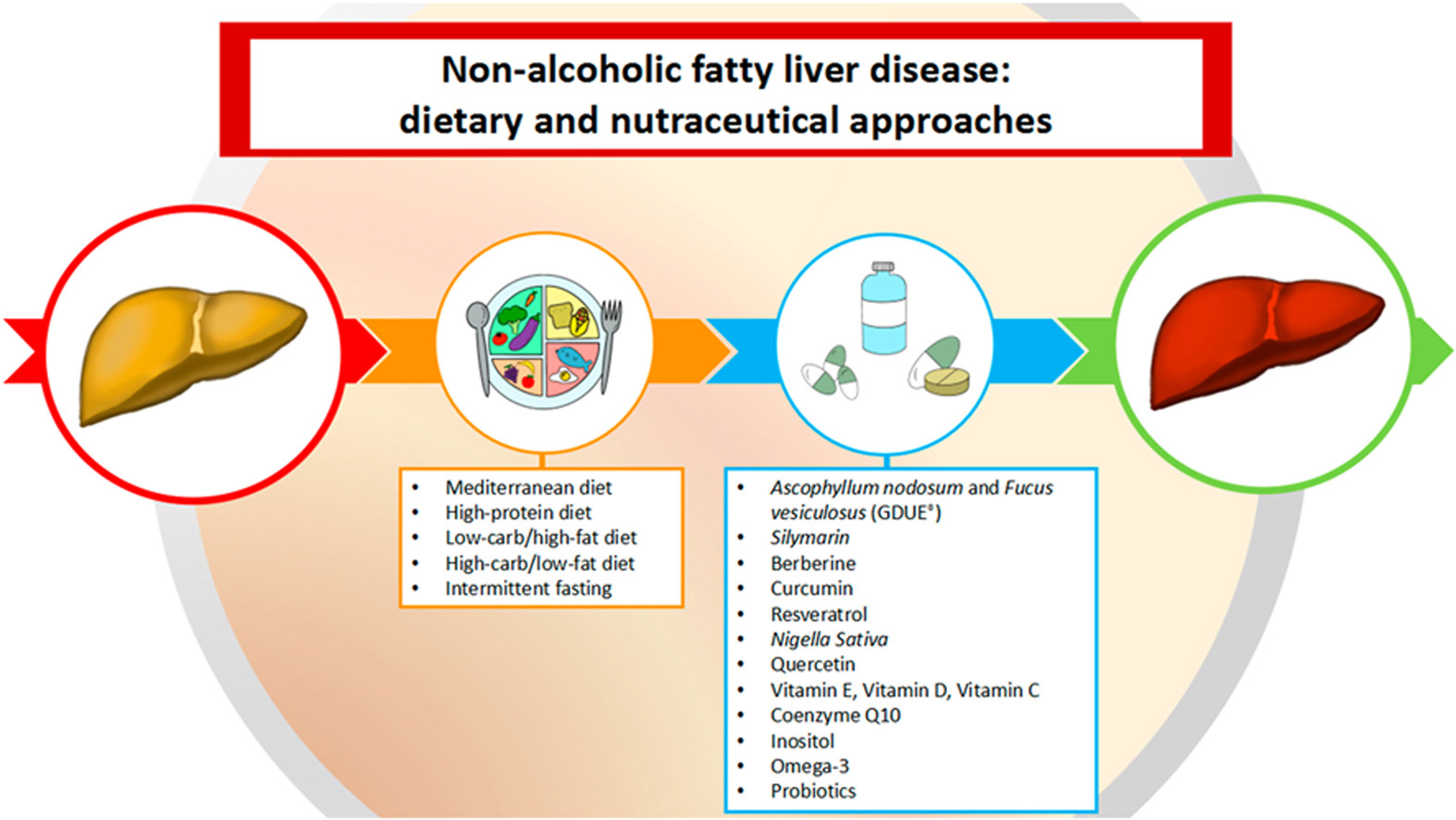
NAFLD – Non Alcoholic Fatty Liver Disease in INDIA; Causes and Nutritional Management of NAFLD
The worldwide prevalence of nonalcoholic fatty liver disease (NAFLD) has increased along with that of obesity over the last decades.
In fact, the global prevalence of NAFLD is around 25%, and it has become the most prevalent chronic liver disease in India also due to its strong association with obesity and lack of physical exercise. Different research reports too peg a prevalence rate of around 20 -25% for Indian population.
The rise in the prevalence of these conditions seems to be largely explained by the exposure to an “obesogenic” environment. This complex and multidimensional scenario is composed of diverse factors that promote an individuals’ overall energy imbalance (i.e., towards a sustained positive energy balance) such as;
- increased availability (food supply) and overconsumption of low-nutrient, energy-dense foods; Food these days is available ‘On Tap’ thus fueling conditions like Obesity and NAFLD
- modern sedentary lifestyle, among others, leading a state of excess adiposity
- Obesity represents the centerpiece in the development of several metabolic complications such as insulin resistance, diabetes mellitus type 2 (T2DM), cardiovascular disease (CVD), and NAFLD
MAFLD – Non-alcoholic Fatty Liver Disease is a multifactorial metabolic disorder in which excessive intrahepatic fat accumulation is the hallmark feature. Occasionally, liver fat is accompanied by inflammation that causes more drastic morphological changes in the liver tissue. It is important to remark that besides over-nutrition, certain types of undernutrition paradoxically may promote the development of fatty liver.
Grades / Stages of NAFLD
NAFLD encompasses a wide spectrum of liver damage that is categorized by histological examination. The least advanced stage of disease, simple steatosis (SS), is characterized by steatosis alone (defined as >5% hepatocytes containing lipid vesicles). Nonalcoholic steatohepatitis (NASH), which represents a more severe form of NAFLD, is defined by the presence of marked inflammation and hepatocyte ballooning with or without fibrosis.
NAFLD is a progressive disease, in which chronic hepatic inflammation is involved in the evolution of NASH to cirrhosis that represents a risk factor for the development of hepatocarcinoma.
How to Manage NAFLD and Hopefully Reverse NAFLD
Healthy lifestyle modifications, namely diet and physical activity, are the mainstay of the NAFLD therapy and nor so much drugs.
NAFLD is part of a complex network of metabolic disruptions in multiple tissues commonly associated with obesity, which consequently makes diet therapy a difficult endeavor.
The present tendency of nutritional intervention leans towards correcting unhealthy dietary factors that promote disease progression. Currently, the optimal nutritional management remains debatable, although there is general consensus that gradual body weight loss is the recommended standard of care for the treatment of NAFLD.
Dietary energy restriction is a key element to achieve weight reduction, but its compliance depends largely on self-control, and consequently, diet adherence might become quite challenging in most cases.
Hence, different choices of nutritional interventions have been explored in the NAFLD context. This write is meant to serve as a comprehensive overview of the most relevant literature describing nutritional/dietary approaches for the management of NAFLD.
Clinical Practice Guidelines – Target Weight Loss
American Association for the Study of Liver Diseases (AASLD) recommends a total weight reduction of at least 3–5% to ameliorate steatosis, whereas improving most of the histopathological features requires a greater degree of weight loss (7–10%).
The European Association for the Study of the Liver (EASL), European Association for the Study of Diabetes (EASD), and European Association for the Study of Obesity (EASO) suggest a 7–10% of total weight loss target. The EASL-EASD-EASO also advises the use of structured programs aimed at lifestyle changes.
| EASL-EASD-EASO | AASLD-ACG-AGA |
Energy Intake | REDUCE by 500 -1,000 Kcal/Day | REDUCE by 500 -1,000 Kcal/Day |
Macro-Nutrient Composition | 4 Diet Types
| Not Specified
Omega-3 Fatty Acids may be considered to treat Hypertriglyceridemia in NAFLD Patients |
Fructose Intake | Avoid drinks and foods with Fructose and added Fructose/ HFCS | Not Specified |
Alcohol Intake | Strictly keep below daily limit of 30 g for Men and 20 g for Women | NAFLD Patients should not consume heavy amounts of Alcohol |
Micro-Nutrients | Short Term usage of Vit E at 800 IU/Day strictly in non-cirrhotic, non-diabetic NAFLD Patients | Short Term usage of Vit E at 800 IU/Day strictly in non-cirrhotic, non-diabetic NASH Patients |
Body Weight Loss Recommendations | 7–10% total weight loss target in Obese / Overweight NAFLD cases | 3–5% total weight loss appears essential in NAFLD cases 7–10% total weight loss target is needed to improve histopathological features in NASH, including fibrosis |
Exercise / Physical Activity | 140 – 200 Minutes/ week of moderate intensity aerobic physical activities in 3 to 5 sessions are preferred, including brisk walking, cycling and jogging Resistance training has shown benefits in promoting Musculo-skeletal strength which helps in metabolic diseases such as NAFLD | Moderate intensity exercise regularly |
AASLD - American Association for the Study of Liver Diseases; ACG – American College of Gastroenterology; AGA – American Gastroenterology Association; EASL - European Association for the Study of the Liver; EASD -European Association for the Study of Diabetes and; EASO -European Association for the Study of Obesity
NAFLD - Plant-based nutraceuticals
Ascophyllum nodosum and Fucus vesiculosus (GDUE®)
GDUE® is a nutraceutical obtained from the brown algae Ascophyllum nodosum and Fucus vesiculosus at a ratio of 95/5; each capsule contains 237.5 mg of Ascophyllum nodosum extract, 12.5 mg of Fucus vesiculosus and 7.5 μg of chromium.
Ascophyllum nodosum and Fucus vesiculosus are rich in natural substances that can slow down cholesterol absorption by increasing intestinal viscosity and also reduce sugar absorption through the inhibition of the α-amylase and α-glucosidase enzymes. It has already been reported that this inhibitory effect is due to the high content of some bioactive compounds, such as polysaccharides, polyphenols, and fatty acids.
Polyphenols act on post-prandial hyperglycemia by slowing down the absorption of carbohydrates. Several studies on GDUE® have reported improvements in parameters correlated with NAFLD. De Martin et al. demonstrated a reduction in HOMA-IR, waist circumference, fasting blood glucose, and insulin levels in overweight or obese patients treated with GDUE®, a capsule taken three times per day before meals for 6 months.
Silymarin
Silymarin is an anti-oxidant agent obtained from milk thistle and at present, silymarin is one of the most-used natural compounds in the treatment of liver disorders, especially in NAFLD, as it has anti-inflammatory, anti-oxidant, anti-fibrotic, and insulin-sensitizing properties.
The recommended daily dosage is between 420 and 600 mg. Silybin is often associated with vitamin E, to ameliorate its effect.
In a double-blind clinical trial, a combination of silybin, phosphatidylcholine, and vitamin E, administered for 12 months, was able to improve HOMA-IR, fasting blood insulin levels, transaminase levels, gamma-glutamyl transferase (GGT) levels, and degree of steatosis at ultrasonography, lobular inflammation, and liver fibrosis in patients affected by NAFLD.
Berberine
Berberine is a quaternary ammonium salt from the protoberberine group of isoquinoline alkaloids and can be found in plants such as gender Berberis. Berberine is known to have lipid-lowering and insulin-sensitizing activity.
A Meta-analysis conducted by Wei et al., that evaluated 501 subjects, proved the positive effect of berberine on lipid parameters, HOMA-IR, and degree of hepatic steatosis in patients with NAFLD.
Curcumin
Curcumin is identified as an insulin-sensitizing and lipid-lowering nutraceutical, extracted from Curcuma longa.
In several studies, a significant reduction was reported in NAFLD-related parameters.
A recent, double-blind, placebo-controlled clinical trial reported that supplementation with 800 mg phytosomal curcumin for 8 weeks led to a significant improvement in fasting plasma insulin, HOMA-IR, waist circumference, blood pressure, TG, HDL-C, liver transaminases, GGT, and fatty liver index in overweight subjects with impaired fasting glucose. A recent Meta-analysis including 16 trials confirmed the positive effects of curcumin supplementation on NAFLD-related parameters.
Resveratrol
Resveratrol is a natural compound, which is produced by several plants under stress to respond to external fatigues or attacks by pathogens.
It is characterized by an important anti-oxidant action, a vasoactive effect decreasing blood pressure, and insulin-sensitizing activity.
Nevertheless, several studies showed a low reduction in liver enzymes in subjects with NAFLD. In a recent Meta-analysis of 7 RCTs, patients treated with 500 mg–3000 mg a day of resveratrol reported no improvement of NAFLD-related parameters. Although a randomized, double-blind, placebo-controlled study using the dose of 500 mg capsule of resveratrol, together with lifestyle intervention, was more effective than lifestyle intervention alone in overweight patients regarding improvements in ALT and hepatic steatosis.
Nigella sativa
Nigella sativa (NS) is an herbal plant, which belongs to the Ranunculaceae family, and its anti-oxidative and anti-inflammatory effects are mainly attributable to its component Thymoquinone.
NS is mainly used in traditional Iranian medicine to treat liver diseases. A Meta-analysis reported that NS supplementation significantly improves transaminase levels, fasting blood glucose, HDL-C, high-sensitivity C-reactive protein (hs-CRP), and degree of liver steatosis compared with placebo.
Furthermore, Saadati et al. conducted a systematic review and Meta-analysis on 7 RCTs in which NS supplementation was proven to reduce BW and total cholesterol, LDL-C, and glucose levels in patients affected by T2DM and MS. Large-sample prospective and randomized studies are necessary to confirm benefits of NS for NAFLD.
Quercetin
Quercetin is a polyphenolic compound with anti-oxidant and anti-inflammation properties. Most studies conducted in vivo and in vitro report that quercetin has hepatoprotective activity against NAFLD, particularly in hepatic steatosis.
Several studies on animal models highlighted the hepatoprotective role of quercetin, reporting normalization of liver enzymes, attenuation of hepatic steatosis, and reduction of total cholesterol, TG, and LDL-C levels.
Vitamins and vitamin-like substances
Vitamin E
Vitamin E is a powerful anti-oxidant composed of a group of eight fat-soluble compounds that include four tocopherols and four tocotrienols.
According to ESPEN guidelines on clinical nutrition in liver disease, vitamin E supplementation is recommended in non-diabetic patients with histologically confirmed NASH to ameliorate liver enzymes and histology.
EASL-EASD-EASO guidelines for the management of NAFLD suggest vitamin E supplementation in non-cirrhotic and non-diabetic NASH patients.
U.S. practice guidelines for the diagnosis and management of NAFLD propose a daily intake of 800 IU/day per os.
A recent Meta-analysis including 8 RCTs reported a significant reduction in transaminase levels, hepatic steatosis, and lobular inflammation in patients treated with vitamin E compared to placebo.
Vitamin D
Vitamin D is a group of fat-Vitamin with well-known anti-inflammatory properties.
Recent evidence suggested that low-serum vitamin D is associated with a high incidence of NAFLD; therefore, its supplementation could improve NAFLD by reducing inflammation and improving IR.
A recent Meta-analysis reported an improvement in HOMA-IR and a reduction in ALT levels in NAFLD patients treated with vitamin D supplementation.
In a randomized, double-blind, placebo-controlled trial, vitamin D supplementation led to a significant reduction in GGT levels in patients with NAFLD.
Vitamin C
Epidemiological studies reported that, in NAFLD patients, vitamin C intake was lower than the recommended daily dose, suggesting an association between vitamin C deficiency and NAFLD.
Indeed, a recent cross-sectional study including 3,374 subjects showed a negative correlation between serum vitamin C levels and the risk of NAFLD.
However, the ESPEN guidelines on clinical nutrition in liver disease do not recommend vitamin C supplementation in NAFLD patients due to poor evidence of efficacy.
Coenzyme Q10
Coenzyme Q10 (CoQ10) is a vitamin-like compound with anti-inflammatory and anti-oxidant properties that was recently considered in the management of NAFLD.
In a recent Meta-analysis of RCTs, it was shown that CoQ10 can regulate adipokine levels and decrease oxidative stress in patients affected by MS.
In a recent, double-blind, randomized placebo trial, the assumption of 100 mg/day of CoQ10 for 3 weeks caused a significant reduction in transaminases, GGT, and degrees of NAFLD; in addition, it improved the adiponectin/leptin ratio, which is related to better glucose control, and a reduction in pro-inflammatory markers, such as IL-6, hs-CRP, and tumor necrosis factor α.
It was shown that the biosynthesis of healthy subjects requires sufficient amounts of CoQ10; however, in various age-related diseases or genetic failure, deficiencies are more common.
Inositol
Inositol is a sugar-like compound that is part of the cell membrane, and two inositol stereoisomers can be distinguished: Myo-inositol and D-chiroinositol. In particular, the latter seems to play a role in insulin resistance; therefore, it may benefit in the treatment of NAFLD, although only limited evidence is available on inositol supplementation in NAFLD.
In a recent systematic review including studies on animal models, it was observed that an inositol deficiency was correlated with an increase in fatty liver, while supplementation resulted in a reduction of hepatic TG and normal liver histopathology.
Large clinical trials on humans are needed to better evaluate the effect of inositol on NAFLD.
Fatty acids
Omega-3
Omega-3 fatty acids are PUFAs in the human diet, characterized by the presence of a double-bond that is three atoms away from the terminal methyl group in their chemical structure.
Although a healthy and balanced Mediterranean Diet can provide a sufficient amount of omega-3 fatty acids, considering their anti-oxidant, anti-inflammatory, and lipid-lowering properties, supplementation may be necessary in some circumstances.
Recent evidence has reported a reduction in liver fat, with omega-3 supplementation, with a recommended dose of 3000 mg/day, but no improvement in NASH degree and liver fibrosis.
A Meta-analysis conducted by Yan et al., reported that omega-3 therapy had a significant beneficial effect on transaminase, GGT, TG, HOMA-IR, and fasting plasma glucose levels. The authors of another Meta-analysis concluded that PUFA supplementation is useful in NAFLD patient management due to the improvement in metabolic risk factors and hepatic markers, but is ineffective for histologic measures.
Probiotics
Microbiome-targeted therapies include probiotics, synbiotics, prebiotics, and fecal microbiota transplantation.
The microbiota appears to play a role in HOMA-IR, obesity, and fatty liver disease. Nutritional and environmental factors could create a favorable micro-environment for bacterial overgrowth and alter intestinal permeability by modifying the degree of lipid infiltration of the liver, influencing the composition of hepatic fat, and increasing pro-inflammatory and fibrotic processes.
A Meta-analysis of RCTs demonstrated that probiotics and synbiotics supplementation, can improve liver steatosis, liver function, transaminase levels, and inflammation markers.
Castillo et al. showed that probiotic supplementation restores the intestinal dysbiosis associated with NAFLD, and reduces liver damage, inflammation, and HOMA-IR; its effect depends on the dosage and period of exposure.
In addition, in the Meta-analysis conducted by Lavekar et al., it was observed that probiotic supplementation resulted in a significant reduction in BMI, ALT, AST, HOMA-IR, and in the ultrasound grade of the fatty liver; however, the authors highlighted that this improvement is not uniform among the studies, due to the different strains (Lactobacillus rhamnosus, Lactobacillus bulgaricus, Streptococcus thermophilus, Bifidobacterium longum) used, the dosage and treatment duration.
Conclusion
NAFLD prevalence is growing alongside that of obesity and it is likely to be so over the next decades. The most effective type of long-term treatment remains diet therapy accompanied with carefully selected supplements.
However, deciding on which diet regimen is best for a patient or group of patients is still a hard task due to the multiple factors that need to be considered. Among the most important features of the most popular diets in NAFLD the following have demonstrated benefits: overall calorie count, food choices, distribution of energy from fat and carbohydrates, and timing.